Demographics:
- Responsible for 5%-20% of cases of pharyngitis in adults.
- Responsible for 15%-30% of cases of pharyngitis in children.
- Most commonly occurs in children between ages 5 and 15 years.
Typical
- Sore throat, pain or difficulty swallowing
- Fever
- Chills
- Malaise
- Headache – frequently frontal in location
- Younger children – abdominal pain, nausea, and vomiting
- Severe unilateral throat pain should raise concern for a peritonsillar or retropharyngeal abscess, especially if this symptom arises or progresses several days after onset of symptoms. Inability to swallow, or odynophagia, should raise concern for a peritonsillar or retropharyngeal abscess.
Typical
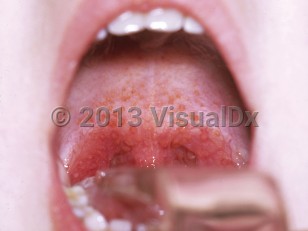
- Pharyngeal erythema
- Exudate (gray-white), tonsillar pillars or posterior pharynx; occasional palatine petechiae, erythema and edema of the uvula, enlarged tonsils
- Anterior cervical lymphadenopathy (classic angle of jaw)
- Scarlet fever – Usually face-sparing, punctate, erythematous, blanchable, sandpaper-like exanthem that may be accentuated in skin folds and creases (Pastia's lines) and may desquamate during convalescence; bright red tongue with inflamed papillae (strawberry tongue); erythematous pharynx and tonsils covered with exudate.
- Children younger than 3 years – Coryza, purulent nasal discharge, excoriated nares (streptococcosis), and generalized adenopathy.
- Exposure to a person with known streptococcal pharyngitis.
- History of acute rheumatic fever or rheumatic heart disease.
- The incubation period is 24-72 hours.
- In most people, fever resolves within 3-5 days and throat pain resolves within 1 week, even without specific treatment.
- Patients with untreated GABHS pharyngitis are infectious during the acute phase and for 1 week after.
- Late winter and early spring are peak GABHS seasons.
Suppurative
- Bacteremia
- Cervical lymphadenitis
- Endocarditis
- Fasciitis / myositis
- Mastoiditis
- Meningitis
- Otitis media
- Perianal dermatitis in children
- Peritonsillar / retropharyngeal abscess (quinsy) – Patient has toxic appearance, "hot potato voice," fluctuant peritonsillar mass, and asymmetric deviation of the uvula.
- Pneumonia
- Sinusitis
- Toxic shock
- Poststreptococcal glomerulonephritis – Hematuria and edema with history of a recent streptococcal infection (elevated anti-streptolysin O titer).
- Acute rheumatic fever – Major (carditis, polyarthritis, chorea, erythema marginatum, subcutaneous nodules) and minor (arthralgias, fever, elevated acute-phase reactants, prolonged PR interval).
- Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS).
- Poststreptococcal autoimmune dystonia secondary to striatal necrosis.
- Poststreptococcal reactive arthritis.
- Sydenham chorea and other autoimmune movement disorders.

 Patient Information for
Patient Information for