Cushing syndrome occurs due to excess circulating glucocorticoids over a period of time. The most common cause is iatrogenic, including the use of topical and inhaled glucocorticoids. Endogenous causes of Cushing syndrome may be divided into adrenocorticotropic (ACTH)-dependent and non-ACTH-dependent disease. ACTH-dependent disease arises when there is increased ACTH from either the pituitary (Cushing disease) or from an ectopic ACTH-producing tumor. Non-ACTH-dependent disease occurs due to either adrenal adenomas or adrenal carcinomas.
Cushing disease accounts for two-thirds of all cases of endogenous Cushing syndrome and is caused by excessive secretion of ACTH hormone by a pituitary microadenoma. This leads to increased secretion of cortisol (secondary adrenal hypercortisolism) from the adrenal cortex as well as increased levels of androgens. The typical cushingoid features seen in patients with Cushing syndrome arise because of the glucocorticoid excess. These cushingoid features are due in part to fat redistribution and typical skin changes.
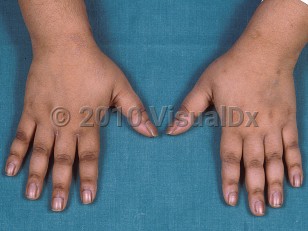
Skin changes in Cushing syndrome are manifold. The skin becomes thin and translucent, and ecchymoses occur following minor trauma. Thinning of the epidermis also leads to the plethoric appearance of the skin. Hyperpigmentation of the skin may be seen but is more common in pituitary or ectopic ACTH production. Although generalized, it tends to occur on sun-exposed areas. Addison disease also results in a similar pattern of hyperpigmentation in sun-exposed areas, but it also occurs in the palmar creases, areas of friction, the vermilion border, genital skin, and the oral mucosa.
Acne, hirsutism, and menstrual irregularities, either oligomenorrhea or amenorrhea, arise due to the increased levels of androgens in Cushing syndrome.
Cortisol hypersecretion also predisposes to hypertension, peripheral edema, glucose intolerance, gonadal dysfunction, osteoporosis, and proximal muscle weakness. Psychiatric symptoms may be present in a large majority of patients (more than 70%), and severity of symptoms ranges from anxiety to mania, depression, and frank psychosis. Insomnia presents early in the disease.
Ectopic ACTH production can also lead to Cushing syndrome. These patients will have sudden-onset hypertension, edema, glucose intolerance, and hypokalemia. Patients with an ectopic ACTH-producing tumor may present with weight loss instead of the typical weight gain. Seventy-five percent of these tumors are small cell lung carcinoma. Ectopic ACTH is produced by bronchial carcinoids, thymic or pancreatic carcinoids, thymic neuroendocrine tumors, medullary carcinoma of the thyroid, or pheochromocytomas.
Patients with carcinoid tumors or pheochromocytomas usually have the typical cushingoid features, as these develop over a longer period of time. Due to the immunosuppressive effects of glucocorticoids, these patients commonly develop cutaneous staphylococcal, candidal, and superficial fungal infections. The incidence of pituitary-dependent adrenal hyperplasia is 3 times more common in women, with the average age of onset being in the third and fourth decades.
Mortality associated with Cushing syndrome is increased fourfold compared with the general population, with cardiovascular disease being the major cause of death. These patients are at markedly increased risk of venous thromboembolism.
Although Cushing syndrome is uncommon in children, obesity along with growth retardation may be a presenting feature in pediatric patients.
This summary focuses primarily on adult patients.
Related topic: pseudo-Cushing syndrome
Cushing syndrome in Infant/Neonate
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
E24.9 – Cushing's syndrome, unspecified
SNOMEDCT:
47270006 – Hypercortisolism
E24.9 – Cushing's syndrome, unspecified
SNOMEDCT:
47270006 – Hypercortisolism
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
Drug Reaction Data
Subscription Required
References
Subscription Required
Last Reviewed:05/21/2023
Last Updated:05/22/2023
Last Updated:05/22/2023
Cushing syndrome in Infant/Neonate