Gardner syndrome (GS) is a subtype of familial adenomatous polyposis (FAP). In addition to the classical finding of colonic polyposis in FAP, GS encompasses a constellation of extracolonic growths and malformations including osteomas, epidermal cysts, desmoid tumors, congenital hypertrophy of the retinal pigmented epithelium (CHRPE), adrenal adenomas, and dental abnormalities.
GS is caused by mutations in the adenomatous polyposis coli (APC) gene and is inherited in an autosomal-dominant fashion. It is relatively uncommon, affecting approximately one in one million people in the United States. Men and women appear to be equally affected, and the disease prevalence appears to be fairly uniform worldwide.
Hundreds to thousands of adenomatous colonic polyps appear, beginning in the second to third decade of life, that will almost inevitably progress to malignancies if not surgically removed.
The osteomas of GS are typically found in the facial bones and carry no significant malignant potential. They range from solitary to dozens in number and from a few millimeters to centimeters in diameter.
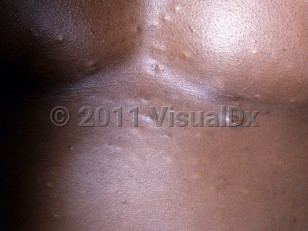
Cutaneous manifestations of GS include epidermal cysts (most common), fibromas, lipomas, leiomyomas, and pilomatricomas. Of note, numerous epidermal cysts can appear early in life and precede the development of colonic polyposis. Epidermoid cysts most commonly occur in the head and neck region.
Desmoid tumors are extremely rare in the general population but affect approximately 10% of patients with GS. They can occur in all musculoaponeurotic structures but are most commonly found in the abdomen or abdominal wall. While desmoid tumors are benign, they are locally invasive and can erode bones, nerves, blood vessels, and hollow organs.
CHRPE is typically asymptomatic. The presence of multiple bilateral lesions can be detected as early as a few months of life and is quite specific to GS.
Dental abnormalities are present in approximately 30% of patients with GS and include hypodontia, unerupted and supernumerary teeth, odontomas, and abnormal tooth morphologies.
Other than intestinal cancer, several other extraintestinal malignancies are more common in GS including duodenal, thyroid, gastric, and pancreatic carcinomas.
Gardner syndrome
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
D12.6 – Benign neoplasm of colon, unspecified
SNOMEDCT:
60876000 – Gardner Syndrome
D12.6 – Benign neoplasm of colon, unspecified
SNOMEDCT:
60876000 – Gardner Syndrome
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
References
Subscription Required
Last Reviewed:08/24/2024
Last Updated:08/25/2024
Last Updated:08/25/2024