Cysticercosis is defined as the systemic invasive tissue infection of the larval stage (cysticercus) of the pork tapeworm Taenia solium. The larva can infect muscle, eyes, brain, and other tissue. There is a frequent misconception that cysticercosis is acquired by eating pork; this is not the case. Human ingestion of pork containing larval cysts of T solium leads to taeniasis, a localized human intestinal adult tapeworm infection. Cysticercosis, on the other hand, is acquired through ingestion of T solium eggs, usually via fecal-oral transmission from a tapeworm carrier (often an asymptomatic food handler or via autoinfection). When cysticercosis involves the central nervous system (CNS), it is known as neurocysticercosis.
Neurocysticercosis mainly affects people living in the developing world but is recognized as a notable emerging infection in the developed world. Although its exact prevalence is unknown, it is endemic in Latin American countries, sub-Saharan Africa, the Indian subcontinent, Southeast Asia, Korea, and China. It has long been regarded as a rare disease in developed countries. However, given advances in globalization and growing numbers of immigrants from regions endemic for T solium, both incidence and awareness of neurocysticercosis have significantly increased in industrialized countries. In the United States, there are an estimated 1000 new cases of neurocysticercosis each year, with most cases reported from New York, California, Texas, Oregon, and Illinois. In a nationwide study examining hospitalization frequency for neurocysticercosis in the United States between 2003 and 2012, Hispanic individuals were at the highest risk, in particular males aged 20-44 years. Sporadic cases involving travel to and from T solium-endemic countries occur in other states as well. The US Centers for Disease Control and Prevention (CDC) considers cysticercosis one of the Neglected Parasitic Infections targeted for public health action.
When food or water contaminated with T solium eggs is ingested by humans, the eggs hatch into embryos that egress into the blood stream through the intestinal mucosa. The embryos lodge in tissues of end organs and transform into larvae (cysticerci). Cysticercal cysts undergo 4 phases of development: the vesicular stage (cyst with a living larva), the colloidal stage (cyst with a degenerating / dying larva), the granular nodular stage, and the calcified stage. Of note, living larvae are only present in the first 2 stages (vesicular and colloidal), and these are the only stages that require and respond to antiparasitic therapy.
In neurocysticercosis, oncospheres (invasive larvae) enter the CNS. Depending on the location, neurocysticercosis is divided into parenchymal and extraparenchymal disease. The extraparenchymal form is further subdivided into ventricular, subarachnoid, Sylvian fissure, ocular, and spinal types. Patients with neurocysticercosis can be asymptomatic. When they are symptomatic, clinical presentations of parenchymal and extraparenchymal neurocysticercosis are distinctly different. Refer to the Look For section for further details.
Parenchymal neurocysticercosis is the most common cause of acquired epilepsy / seizure in endemic areas. Seizures can develop when the cysts are in viable or degenerative stages. Depending on the location and the number of the cerebral parenchymal lesions, patients can present with motor or sensory deficits, language difficulty, parkinsonism, or lacunar or large cerebral infarcts from cerebral ischemia or cysticercosis angiitis. When there is an intense inflammatory response around the cysts, patients become comatose, obtunded, or encephalopathic (cysticercosis encephalitis).
Extraparenchymal neurocysticercosis presents with symptoms of increased intracranial pressure and hydrocephalus from blockage of cerebrospinal fluid (CSF) outflow tracks by ventricular cysticerci. In cases of intraventricular neurocysticercosis, 2 syndromes are of note: Bruns syndrome and double-compartment hydrocephalus syndrome. Bruns syndrome is characterized by episodes of sudden loss of consciousness related to head movements when cysts in the 4th ventricle cause intermittent obstruction of the cerebral aqueduct by a ball-valve mechanism. Double-compartment hydrocephalous syndrome is defined as both 3rd and 4th ventricular dilatation secondary to the simultaneous obstruction of cerebral aqueduct and foramina of Luschka and Magendie by intraventricular cysts. Symptoms of headache, nausea, vomiting, or dizziness are common.
Cysticerci within the subarachnoid space of Sylvian fissures or CSF cisterns can develop into multilobulated grape-like clusters, known as racemose cysticercosis. These lesions are usually larger (> 10 cm long) and can occlude the foramina of Luschka or Magendie, causing obstructive hydrocephalous. The condition can also cause basal meningitis or arachnoiditis with cranial nerve entrapment presenting as visual field defects and cranial nerve palsies.
Spinal neurocysticercosis is rare, and patients typically present with paresthesia, radicular nerve pain, or bowel / urinary incontinence or retention.
Ocular neurocysticercosis can involve the subretinal space, vitreous humor, anterior chamber, conjunctiva, or extraocular muscles. Subretinal ocular cysticercosis is considered to be a form of neurocysticercosis, whereas involvement of the anterior chamber of the eye alone is regarded as extraneural cysticercosis. The clinical manifestations of ocular cysticercosis are eye pain, impaired eyesight, or double vision, depending on the involved structures.
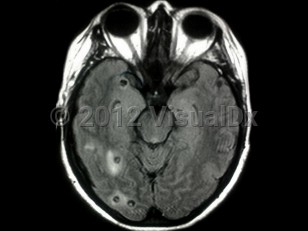
Neurocysticercosis
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
B69.0 – Cysticercosis of central nervous system
SNOMEDCT:
230215006 – Cerebral cysticercosis
B69.0 – Cysticercosis of central nervous system
SNOMEDCT:
230215006 – Cerebral cysticercosis
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
References
Subscription Required
Last Reviewed:02/01/2022
Last Updated:02/02/2022
Last Updated:02/02/2022